Fat women of color have been leaders in almost every political movement to end oppression. Appreciate and recognize their labor.
Also notice how Coulter is using fatness to derail the conversation away from the issues being raised by the protesters. Notice how she is using fatness as coded language to discuss the “problem” that women of color pose to the white supremacist establishment. Anti-fat bigotry is rooted in racism and white supremacy, and this tweet is a perfect example of that evil union.
“I still have bad thoughts about myself, but I’ve learned that you have to love yourself the way you are,” Robles says. “I may look like this, but I’m in the Olympics because of the way I am.”
It’s 2015. If doctors don’t know how to operate on fat bodies. Then they shouldn’t be doctors. We have enough resources an equipment to deal with “obese” patients. There is no need for the medical community to continue fat shaming.
Let’s talk a little bit more in depth about how obesity affects surgical procedures.
In most serious, intensive surgeries, you’re probably going to be under anesthesia, right? And you’re probably going to have medications to take afterwards. Stuff like this filtered through the kidneys and liver.
Obese patients have much higher rates of renal hypertension, which affects the kidneys, and morbidly obese patients have a 90% likelihood of having abnormalities in their liver.
That all adds up to a really bad time, and drugs being filtered out of the system quicker and therefore not working as intended. And you really want your anesthesia to work right when people are cutting into you.
In addition to this, some weight-based drugs are affected by fatty tissue, and some are not, so this can cause problems in determining the proper dosage.
Obese patients are at a higher risk for deep-vein thrombosis – this is when a blood clot forms in a deep vein, like in the leg. Surgery is recognized as a risk factor for DVT, and so obese patients undergoing surgery are doubly at risk.
Finding veins in the patient is also made difficult – it’s the difference between finding the edge piece in a 1000 piece puzzle, vs finding it in a 100 piece puzzle.
It’s harder to monitor blood pressure in obese patients as well, as standard cuffs may not work due to there being too much fatty tissue between the blood vessel and the cuff.
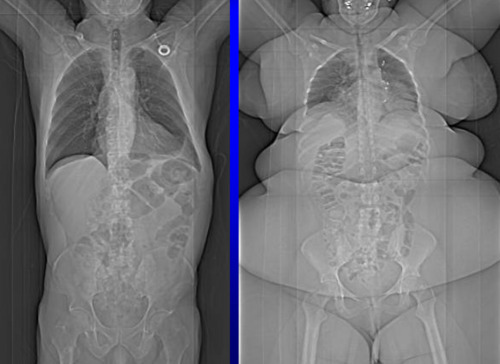
When you’re performing surgery, you have to pull back the flesh and muscle to get to where you’re trying to operate on – the more you have to pull back, the more difficult this becomes.
This image shows how much more you’re having to work through when doing an operation on an obese person:
So no, it’s not a matter of doctors being bad at their job. Surgery by itself is a difficult and risk-laden process – adding obesity on top of that adds an uneccessary layer of additional risk and complexity.
Sources:
Palmer M, Schaffner F. Effect of weight reduction on hepatic abnormalities in overweight patients. Gastroenterology 1990; 99: 1408–13.
Albert S, Borovicka J, Thurnheer M, et al. Pre- and post-operative transaminase changes within the scope of gastric banding in morbid obesity. Schweiz Rundsch Med Prax 2001; 90: 1459–64.
Ramsey-Stewart G. Hepatic steatosis and morbid obesity. Obes Surg 1993; 3: 157–9.
Clain DJ, Lefkowitch JH. Fatty liver disease in morbid obesity. Gastroenterol Clin North Am 1987; 16: 239–52.
Marik P, Varon J. The obese patient in the ICU. Chest 1998; 113: 492–8.
Ribstein J, duCailar G, Mimran A. Combined renal effects of overweight and hypertension. Hypertension 1995; 26: 610–5.
Braekkan SK, Siegerink B, Lijfering WM, Hansen JB, Cannegieter SC, Rosendaal FR. Role of obesity in the etiology of deep vein thrombosis and pulmonary embolism: current epidemiological insights. Semin Thromb Hemost 2013
Allman-Farinelli MA. Obesity and venous thrombosis: a review. Semin Thromb Hemost 2011; 37:903-7.
This is very true. When I had open heart surgery, there were various complications as well as problems with the anesthesia because of how fat I was. Thanks be to God my surgeon was top notch. But the fact of the matter is that if I was a thinner patient, the surgery would have been far less traumatic. In fact, if I had not put on so much weight, my aortic valve would have lasted me longer. So, yeah, biological and scientific realities are at stake when you carry too much weight.
I have seen some communities on tumblr try to push a “body positive” self esteem agenda by dismissing health risks of obesity as fat bias.
Yes. You can be beautiful no matter what your body looks like.
No. You cannot always be healthy regardless of what your body looks like, and while self confidence is important, taking care of yourself and addressing health problems-including being overweight- is important.
Thanks for someone being honest and real about the risks of obesity and the medical field
Im glad this didnt explode and now ive learned a little more about health risks and obesity. Thank you tumblr
No.
This is still wrong. If fat bodies are harder to operate on, metabolize anesthesia at different rates, if fat bodies are less healthy, that is irrelevant.
Doctors should LEARN how to treat fat people, because they should learn how to treat all their patients. If they can’t deal with somebody who diverges from the figure in the high school anatomy textbook, then they are BAD doctors.
Obese people are less healthy, you say? ..if so, what DIFFERENCE does that make? People generally come to a doctor when they have a HEALTH issue.
If somebody has an appendix threatening to burst, you, as a person with many years of medical schooling, should have a more immediate, practical answer than “lose some weight.”
If doctors are so bad at operating on fat bodies, because they have different anesthesia needs or more folds to cut through, well then maybe medical schools should train them to provide life-saving treatments to people who aren’t calvin klein models.
People can be obese but metabolically healthy and fit, with no greater risk of developing or dying from cardiovascular disease or cancer than normal weight people, according to the largest study ever to have investigated this seeming paradox
Of course fat people have been saying the same thing for decades. But of course anything a fat person says about themselves or their own health is laughed off as “wishful thinking”. Our own experiences are constantly being denied as “head in the sand” “it will catch up to you eventually” mentality. Despite those of us that exercise regularly and eat healthy, we’re told that none of it matters because we’re still fat -and therefore couldn’t POSSIBLY be healthy.
The sad thing about it though, is that people should not have to be healthy in order to deserve to be treated with human decency and respect and not have to live their lives stigmatized, bullied, marginalized, and shamed. People are deserving of equality and respect reguadless of if they are healthy or not.
You know that the real pisser is, though? There’s absolutely no medical evidence that most of the common metabolic disorders that are associated with obesity are actually caused by obesity in the first place. No one has ever been able to conclusively demonstrate a causal mechanism – correlation is all we’ve got. It’s entirely possible that we’ve got it completely arse-backwards; i.e., that it’s the metabolic disorders that lead to a greater propensity for obesity, rather than the obesity that leads to the metabolic disorders.
Exactly. The study identified a sub-group of fat people who were just as healthy as thin people. These fat people were
“metabolically healthy”. But no causal connection has been proven that obesity causes metabolic disorders. So no, there is no blaming the metabolically unhealthy fat people for their issues. And even if there were, fat people deserve to be left the fuck alone. This shit is between fat people and their medical team. It is not an excuse for the rest of the world to point fingers.
This was also interesting:
In an accompanying editorial on both papers [3], Stephan von Haehling, Oliver Hartmann and Stefan Anker conclude: “The available studies, together with previously published study data, permit the conclusion that weight loss in patients with chronic illness and a BMI <40 kg/m2 is always bad, and in fact not a single study exists to suggest that weight loss in chronic illness makes patients live longer. In this context, fat tissue has several beneficial effects, for example in its action as an endocrine organ, but also, nevertheless, as an aid in protecting against hip fracture. Obesity may carry benefit up to a certain degree, and it should be recognized that obesity is not necessarily associated with abnormal metabolic function.”
Weight loss in chronically ill people who are fat but not super-duper fat is always bad and there is no reason to harass them to lose weight.
I say that again:
Weight loss does not help chronically ill fat people become healthy, and in fact provides certain protections that confer longevity.
At some point people are going to have to admit that it’s not about our health, it’s about finding our bodies distasteful.
If naysaying, nagging, concern-trolling assholes really cared about our health, they’d campaign to make sure that all fat people had access to good, affordable, evidence-based health care, as well as nutritious food that meets each individual’s specific health requirements.
In general, though, your confusion comes from the over-simplified myths about weight that permeate our culture.
First, fat is not only an energy storage device, it is also an important endocrine organ. This means that the fat organ regulates hormones, and thus, helps to regulate the functioning of many other organ systems in the body. So the fat organ can grow in response to non-food-related factors, like chronic stress or sleep deprivation, as part of the body’s adaptive response to those factors. (And guess what is stressful? Dieting and weight loss.)
Second, when people do not consume enough energy to meet their needs, two biological processes are triggered. The first is catabolism, which is the process of breaking down the body’s cells to release the energy and nutrients stored in those cells. That energy is then used to fuel the body. This is what people usually think happens when people restrict their food intake to lose weight: the body breaks down fat for energy. Of course, when catabolism does happen, fat calls are not the only cells that are broken down: the body also breaks down muscles, organs, bones, and ligaments to access necessary nutrients and energy. (Yikes.)
But the second process that is triggered by an energy deficit is metabolic suppression: The body slows down all the basic, life sustaining processes of the body to conserve energy.
So a person can gain weight while restrictive dieting because an energy deficit causes the body to slow all the life sustaining processes of the body in favour of growing the fat organ, which helps the body to survive in times of stress.
This is some serious shit, people, and it’s a big part of the reason that intentional weight loss through restrictive dieting is so unhealthy.
so if the metabolism is slowed, how does that impact the energy deficit? does it mean less calories are “needed”? because that could work out, stating probably too simply, that if less energy is being used then there is more excess to store as fat.
and if fat growth is happening despite restriction, is catabolization happening?
(sorry if you cant answer these)
“so if the metabolism is slowed, how does that impact the energy deficit? does it mean less calories are “needed”?
Weight loss is often framed that way: Oh, your metabolism is slowed, so you don’t *need* as many calories as other people need! Just keep eating less and you will maintain your smaller body!
But maintaining your body in a state of suppressed matabolism is not a good thing. It literally means that your body has instituted emergency measures to survive. Any non-essential physiological processes – like the reproductive system – are dramatically slowed and can be stopped completely. And even essential bodily processes like the transmission of fluids into and out of cells (the most basic biological function), to the regeneration of cells, to the functioning of the immune system, to the re-myelenation of nerves (essential for their function) are all slowed down.
This is literally what it means when the sources I linked above say that the basal metabolic rate is slowed by weight loss: The body is slowing down all of its essential, life-sustaining physiological processes in order to survive. That is not a good thing. It is not a state that any organism can or should sustain in the longterm.
PS: And yes, when those basic processes are slowed, it can “free up” energy to grow the fat organ.
And, yes, catabolization (destroying body cells, a very bad thing to happen in case you haven’t guessed) still happens when you don’t eat enough even if you’re fat!
Thank you for adding this. My post was not clear enough on this point: Even if many fatter people’s bodies favour metabolic suppression in response to an energy deficit, catabolism can and does still occur if they do not eat enough. It’s just that rather than catabolizing fat cells, their body will destroy other cells to meet energy needs – including the cells in muscles, ligaments, organs, and bones – which can lead to serious health complications in the long term.
I often wonder how many of the so-called diseases of “obesity” are actually caused by chronic dieting and disordered restrictive eating. Chronic undernourishment and weight cycling are related to so many “fat diseases,” including GERD and other stomach and digestive issues, cardiovascular disease, pancreas and gall bladder diseases, and even premature death.
This is true. I saw a documentary about it. Men’s orgasm faces are allowed in teenage comedies rated PG13, but women’s orgasm faces can often push it into NC-17 territory, no joke.
This is pretty much the equation:
women receiving abuse = PG-13/R
women receiving pleasure = R/NC-17
Ugh. I did a speech on this shit, and watched the documentary about it. Pisses me the fuck off.
So absolutely ridiculous. Yes, please, show us being raped, murdered, mutilated; but don’t you dare show us engaging in sexual gratification. Because that would be…obscene.